
Photo of the Soufrière Hills volcano on Montserrat in 2004 with summit obscured.
(photo provided by Dav Macfarlane) |
Eruptions and disasters
|
Photo of the Soufrière Hills volcano on Montserrat in 2004 with summit obscured.
(photo provided by Dav Macfarlane) |
Chris and I had enjoyed the MM-Wave Group’s Christmas party and our Christmas day in 1997. However after Christmas things started to go downhill and life gradually became more difficult for us both during the following years.
On Tuesday 30th of December 1997 we went on a shopping trip to Edinburgh. In part this was just to have a day out and see what we might fancy from the shops. But one specific aim was that Chris wanted some new shower curtains. We had managed to get some information about shops in Edinburgh before we went. Unfortunately it started to rain quite steadily by the time we arrived, and the information was misleading. The result was that we ended up walking the length of Princes St from Waverly Station, searching for a specific shop we were unable to find. This in itself meant we got wet. But when at our furthest from the station Chris had a bad fit at about 1:30pm.
I managed to prevent her from falling, but had to lower her onto the pavement where she was, of course, laying on the wet paving as more rain poured down. Our umbrella wasn’t able to cover her completely. Fortunately a couple of passers-by helped me keep her on her side. After a few minutes I realised that the people around us had made a canopy over us with their umbrellas, sheltering us from most of the rain. Alas, someone with a mobile phone called for an ambulance. I had explained that by the time any ambulance came she almost certainly would’ve got up and walked off in an ‘automatic’ phase. This was a common feature of her fits. During this phase she can’t understand when someone may try to stop her walking off, and insists on marching away. So when she did get up I had to chase after her, calling out to the others that she’d be OK and to apologise to the ambulance crew. About ten minutes later I heard an ambulance, but by then we were both a long way from where the fit had occurred, so couldn’t explain. I had to keep with her in case she panicked or did something dangerous. When she’d recovered she felt tired and confused, so we abandoned the shopping and came home.
I was grateful to the people who helped, and never got a chance at the time to thank them properly. So if you were one of them, thanks!
By the beginning of 1998 Duncan Robertson and I had seen our first NERC grant proposal rejected and had started to put together a new application. Our interest in volcanology had initially been sparked some time before by one of those chance events that provided an opportunity. Professor John Shepherd was an established volcanologist, and he’d visited the St Andrews Physics department because his daughter had started an undergraduate degree here. As a visiting academic he was welcomed and I, along with other staff, had a chance to meet him and chat over a cup of tea.
By that time I’d developed a habit of asking visiting scientists questions along the general lines of: “What kind of measurements or observations would you like to be able to make, but haven’t been able to find a way?” I’d realised some years before that this was a key question because in practical terms, physics is the science of measurement. And as someone who adopted an engineering approach to questions, my interest was in devising ways to make better or more accurate measurements possible. Since I knew nothing about volcanology I was curious to find out if a suitable application of mm-wave technology might help. What John said was so interesting that we then went down to the mm-wave lab and I showed him the kind of equipment we were making. Duncan and I then had a more detailed discussion with him about what observations volcanologists wished would become possible.
The main points which emerged from what John said were that:
In essence, the basic problem was that whenever something ‘interesting’ was happening, volcanologists usually couldn’t actually see it because it was shrouded behind clouds of dust and smoke! Given that it was also too dangerous to actually get close when a volcano was active, they were seriously handicapped when it came to examining extremely active behaviour. Even when a volcano wasn’t ‘active’ in the layman’s sense of erupting violently, it might often be venting hot gases and vapours which also could cloud the view. And in addition, the summit and other high altitude parts might often be hidden by meteorological clouds. The result was a catalogue of unwanted obscurations, impeding observations or measurements. Duncan and I quickly realised that this was, in fact, an almost tailor-made application for mm-wave sensing!
An established tactic in battles is to ‘make smoke’ so the enemy can’t see you. Most people will have watched a film or TV programme where a ship does this to hide behind so an enemy warship can’t aim its guns at them. The same tactic is also used on battlefields. In most cases the ‘‘smoke’ consists of a cloud of particles which are small enough to float in the air. However the level of obscuration depends on the relationship between the size of the particles and the wavelength of the electromagnetic radiation used.
|
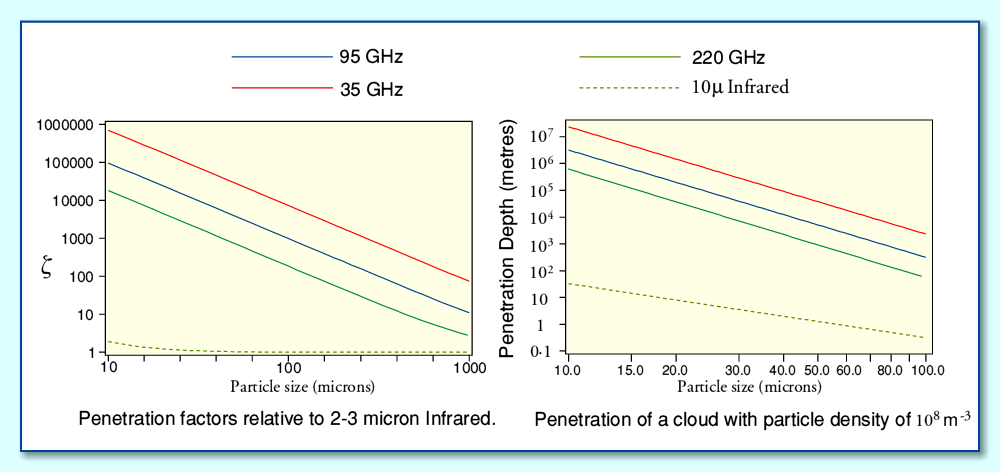
The above graphs indicate how – by choosing to make observations at longer wavelengths – we can see though clouds which totally obscure the view from human eyes. Visible light has a wavelength of less than 1 micron (millionth of a metre). By using cameras, etc, that can detect Infra-Red radiation at longer wavelengths it becomes possible on a battlefield to see though smokescreens of particles that block human vision. The graphs therefore include as a reference the use of 10 micron IR radiation, and this works well for clouds of very small particles that stay suspended in the air for a long time. Larger particles tend to fall out of the air more quickly, so tend to clear away too rapidly to be useful on a battlefield. But an active volcano may keep emitting large clouds of these large particles, refreshing the number floating in the air. Thus maintaining its smokescreen. As a result a conventional IR sensor or camera may become useless for observing the volcano.
By moving to millimetre wavelengths we can dramatically improve our ability to see though such clouds. For example, if the particles that make up a cloud have a typical particle size of 30 microns, we can see through a cloud that might be many thousands of times too thick or deep to see though at visible wavelengths. Very large particles – or flying rocks! – might still block the view, but tend to fall out of the air quite quickly!
Looking at the above graphs the implication is that it makes sense to go for the lowest frequency in order to maximise the ability to see though clouds of dust. However that has a drawback...
|
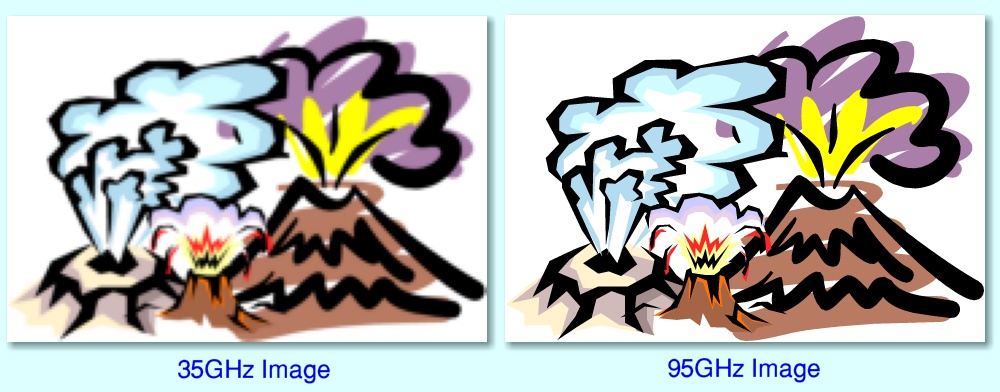
The resolution – i.e. how much detail we can see when producing an image – depends on the ratio between the size of the instrument optics and the chosen wavelength. Hence, for a given size of instrument optics, 35GHz will produce a much less detailed result than using 95GHz. The above images indicate the extent to which the image becomes more ‘blurred’ as a result. Hence in practice there is a trade-off between the ability to see though clouds of dust and the ability to obtain detailed images. We’d like to use a low frequency to see though dust, but prefer a high frequency to gather detailed images. In principle we could make a bigger system with larger optics to improve the situation. But in reality avoiding an excessively large or heavy instrument is particularly desirable in an ‘out in the field’ application like volcanology given the potential danger involved!
Duncan and I knew that two standard mm-wave techniques would be very useful for volcanological observations:
We also realised from the start that it should be possible to combine these two techniques into a single instrument (usually called a ‘radarometer’) that could provide a three-D video ‘map’ of the volcano’s surface shape and temperature and how it evolved. But of course, we needed to first show that we could walk before trying to run!
Our first proposal to the relevant research committee had been rejected in 1997. But we decided to have another go and submit an improved application, along with a number of volcanologists we’d started to co-operate with. By early 1998 both Duncan Robertson and Graham Smith had in practical terms moved on from being postdoctoral researchers working for me. Graham was now a Research Fellow, and worked mainly with Professor Peter Riedi. In effect, he was now the driving force for an entire new area of research based on the initial mm-wave ESR system. Duncan was by this time doing the Lion’s share of the work on the systems we had been developing for DERA, and preparing the proposals for volcanology. My role had changed.
I had effectively ceased being involved with Graham’s work. I was still doing a fair amount of ‘theoretical study/analysis’ work to help Duncan decide how to optimise the proposed design for a volcanological scanner. But in reality Duncan’s contribution was much greater than mine. I was mainly acting as a consultant to advise/help/support him, not the other way around. During 1998 other developments also occurred and over a period of time the members of the group of volcanologists involved in the proposal to build a mm-wave scanner also changed.
To a large extent ‘handing over’ of the work to Graham and Duncan was to be expected. They had become the real experts in the areas they worked on full-time. I was having to do a variety of other tasks. For example, in addition to having other research students I was still acting as the supervisor for Natalie Ridge and her work for DERA. During 1998 this involved a number of visits to St Andrews by her sponsors, coming to see progress and decide what direction to take. However Chris had become increasingly unwell and we both found this increasingly difficult to deal with. It wasn’t her epilepsy, but for many years neither we, nor any of the GPs or consultants we saw correctly diagnosed it. The result was a lack of appropriate treatment. Indeed. as events unfolded the way she was medically treated would often make things far worse, not better.
Most of the time Chris was busy, active, and outgoing. She continued to regularly go to long meetings of the FHC (Fife Health Council) and other NHS related meetings. However she also had started to go though periods which lasted from a few days to a few weeks when she felt unable to go out at all or see anyone. During these times she tended to spend a lot of time in bed, sleeping. But when up or awake became quite depressed or anxious. As the months passed these ‘down’ periods became longer, more intense, and the levels of anxiety and negativity would become quite severe. Her general feeling would be that everything was hopeless or terrifying and she was unable to do anything or see anyone because it was too difficult or frightening. In contrast, when she felt ‘up’ she enjoyed socialising, challenging authority at meetings, pushing for improvements, helping other people with their problems, etc.
When in a ‘down’she was also at her worst during the early mornings. One consequence was that between about 3am and 8am she found herself unable to sleep because she felt so frightened, anxious, and depressed. She would then wake me up. Sometimes to ask me for help to calm down. But increasingly often to tell me that everything was hopeless, and she’d never feel any better or be able to do anything again. When in this state of mind I quickly learned I had to talk to her with great care regarding exactly what I said or my tone of voice because she would become angry and more anxious if I tried to simply convince her that she would feel better later on and be able once again to do the things she wanted to do. The problem was at such times she felt absolutely certain that things were now hopeless. So any attempt to say otherwise was essentially denying how she felt.
Later on the same day she would usually get up, and gradually feel better. Often, by the evening she was more cheerful and frequenctly apologetic for how she had felt and behaved in the early morning. But we would then probably go though the same pattern of being ‘down’ in the early morning and ‘recover’ during the day, every day for some time. Then this behaviour would evaporate – only to return again weeks later.
Although variations in her mood had occurred for years, they grew worse once the St Andrews CAB was shut down and replaced by CARF. This took away a routine where she could go a number of times each week and work with friends to meet other people and help them deal with their problems. Helping people at the CAB showed Chris that she was doing something useful. She felt that CARF was totally different in the way it operated, and she doubted it helped most of its clients. The scope for volunteers to do the work was relatively limited and formulaic. During January 1998 Chris started inquiring about working for the CAB in Dundee. This was in Tayside Region, so beyond the scope of Fife Council’s decision to axe the Fife CABs.
The ‘down’ pattern of mood and behaviour was very bad for Chris. But it also meant that I was losing sleep whilst being required to keep up with my work at the University. During ‘downs’ when I had to go to work I worried about Chris being OK at home because her mood was at times becoming suicidally depressed, confused, and anxious. Duncan and the others I worked with became aware of the problems because I didn’t attempt to keep them secret. They sympathised, and helped so far as they could, but of course I still needed to support their work as required and to do my own work as paid for by the University or DERA as effectively as I could manage. One particular side-effect of the worry was that I became more and more anxious about travelling away from St Andrews without Chris unless I was certain she’d be OK whilst I was away. Inevitably, my failure to attend some meetings did have a negative effect on making progress with some of the work Duncan and I wished to get funded.
At the time Natalie was working on developing a novel form of antenna for use as part of a project to build an improved landmine detector. There had been a significant change in the way mines were constructed. Instead of being made with a metal casing and mechanism, newer designs used polymer and ceramic materials. This let them avoid being found with conventional mine detectors which relied on sensing the metallic parts of the object. Good news if you were laying mines to prevent an enemy from reaching you. But very bad news if you were a third-world farmer or one of their family members in the years after a war had been fought in your area. Many civilians were being killed as a result of undetected – and almost undetectable – mines which had been scattered and left without their locations being recorded. So there were more than just good military reasons for finding a way to detect these mines!
The method being developed was to employ NQR (Nuclear Quadrapole Resonance) to detect the explosive material inside the mines. In general the explosives used Nitrogen compounds that show a characteristic resonance of this type. But the response was quite weak, difficult to detect, and relied on a system that would stimulate the resonance by applying the correct ’driving’ field as well as picking up the response. Natalie’s task was to develop an improved ‘antenna’ or coupling system to make this possible for a portable system. The technique she used was based on surrounding the antenna with a ‘sheath’ of plasma – ionised gas at low pressure. The system was encapsulated in a glass surround to obtain the required low density gas layer to be ionised whilst in use.

The above photos of a Soufrière Hills volcanic eruption illustrate
how the clouds of dust, etc, released can obscure the view! |
I can’t now recall exactly when it happened, but I do remember one interesting day when the DERA sponsors of this project flew up to St Andrews with a ‘dummy’ plastic mine for us to conduct a field test... or more accurately a ‘beach test’ because we carried it out on the West Sands at St Andrews. All the plastic/ceramic parts of the mine were those of a then-common design used to make real mines. But the explosive had – at least so I was told! – been replaced by a ‘similar’ compound that was inert but which exhibited the same NQR properties as the genuine explosive.
We divided into two groups, and one group buried the mine without the others seeing where it was. The other group then used an experimental detector to try and find it. Alas, this effort failed. This wasn’t a great surprise as it was an early test, but we then realised that the group who’d buried it also weren’t sure where it was! So we spent some time digging holes searching for it. At this point I was wondering what would happen if we had to give up and leave it. Thus ensuring that at a later date some holidaymaker or merry golfer would discover it and raise an alarm. Then have embarrassed MoD people admit it was “one of ours” and not to panic! Fortunately, we found it. Just to cap the day, when the MoD people went to Edinburgh airport to fly home the checkin staff noticed the dummy mine and refused to allow it onto the plane, regardless of official assurances it was safe. So it had to make its way home to Fort Halsted by other means...
By a quirk of history, this wasn’t the first time St Andrews had played a part in the development of detecting land mines. The inventor of the original mine detectors had used the St Andrews beaches many decades earlier to test their effectiveness.
In March 1998 the head of the Physics Department and I were both chasing the University to ensure that Graham’s success would – as they’d promised – lead to a lectureship. Although this was expected, the University hadn’t actually stated that it would occur, or when. More frustrating was that Duncan was only being employed by a series of DERA contracts, each lasting a year or less. The people at DERA who sponsored his work always assured us that we could expect continued funding, but this could never be formally established. The result was that Duncan’s status was such that the University and UK research councils would not allow him to apply for research grants. Instead, anything he did had to be as if I were the person who was responsible. And, unlike Graham, his work wasn’t somehow seen as being as ‘academic’ when it came to any possible consideration for a job as a permanent academic. Frankly, this was absurd, infuriating for me, and frustrating for him. But “them’s the rules” was the stubborn attitude of the University and research councils.
In April 1998 Chris started investigating the possibility of standing as a candidate for the St Andrews Community Council (StACC). This might well be a way to help people by airing their problems and to foster campaigning to help deal with them. By this time Chris anticipated working at the Dundee CAB, but wanted to have a more local involvement in community activity to help others, and in the process combat her periods of depression and anxiety.
In May, Chris’s GP started her taking a ‘new’ medication for her fits. The main result was as I outlined in an email from home to Dave Walker of ‘Acorn Computers’ shortly afterwards.
|
Sorry again about the delay reacting to your e-mail. Chris has been ill this last week. (Now largely recovered.) You *may* remember that she has epilepsy. This isn't normally much of a bother, but every now and then we get a 'bad week or two'. Last week she had some fits that gave the effect of making her *really* frightened. To the point of screaming and shivering. Not nice - *especially* for anyone who doesn't know that, in fact, she is 'unconscious' and has no real idea what is happening. It is all on 'autopilot' and she doesn't remember it half an hour later. ...
The upshot was I spent 90% of last week at home with her as she was frightened of my leaving her. Hence I missed your e-mail (which went to my university address) until this morning. |
I also emailed Duncan from home to keep him informed, having not been into the Physics dept for days, and to let him know I also had to go to Dundee with Chris to see her epilepsy/neurology consultant, admitting that I felt a “bit shattered” by the events of the previous week.
After a few days of this particular episode I found out that the ‘new’ medication was actually carbamazepine – which had in the past caused Chris to become anxious and confused! Unfortunately I’d not been told about the details of the change and – as was usual at the time – I didn’t go with her to see the GP. Once I realised what had happened we decided she should stop taking it and revert to her previous regime. The GP had presumably hoped the change would help, and hadn’t checked the medical history but in practice, it made things worse.
By mid 1998 I’d written a number of magazine articles for various specialist magazines about Acorn Computers and their uses. I had also got to know some of the people who developed hardware and software for the machines, and often chatted with Dave Walker and various other people about the topic. Dave and I shared a common interest in high quality Hi-Fi equipment and malt whiskies as well as Acorn computing! Acorn had announced their planned new ‘workstation’ home/office computer which had become known as Phoebe. The name was given to it in homage to a character in the American TV series, ‘Friends’ and initially signified that – as yet – it wasn’t well endowed with brains! I’d actually pre-ordered one as an upgrade to the Acorn RiscPC machines I was using at the time.
Dave and I were having regular discussions because I was trying out the ‘Java’ system Acorn were developing. At the time Java as a computing language (often wrongly confused with the totally different Javascript language) and the concept of a ‘Java Virtual Machine’ (JVM) was aimed at allowing programmers to write a program that could then run on any computer hardware and OS which provided a JVM. In addition, an independent developer, Peter Naulls, was also independently developing his own JVM/Java system he’d called !Chockachino, and I was also beta testing that on my Acorn Risc machines. The tests let me create some simple programs and ‘applets’ as well as give them feedback to improve what was being developed. Alas, ultimately, neither the Phoebe computer, nor either RISC OS JVM ever really appeared. And to be honest, my personal view of Java eventually became that it was like trying to learn chinese whilst people kept changing the glyphs at random as fast as you learned some of them. So I’m still writing programs in ‘C’...
On 1st June 1998 Chris joined her first StACC meeting having been elected as a Community Councillor. A few days later I had a visitor from DeBeers, the diamond company. This was the start of a set of meetings, emails, etc, as we explored the possibilities of using mm-wave scanners to detect diamonds for industrial and security purposes. These went on for a few months but didn’t lead anywhere. So alas, I never did see any diamonds as a result.
By June, having joined StACC, Chris decided that she would prefer to cease being a member of Fife Health Council. This was for various reasons. The main one being that many of their meetings were difficult for her to attend, often starting at 9am in a location like Glenrothes. Because she has epilepsy she can't drive a car. So it meant a combination of some long walks and more than one bus journey, leaving well before 9am. During these trips, she often had a fit. She had also reluctantly come to the conclusion that the FHC was largely a waste of effort. Having served on it for a few years she’d come to feel that it didn’t really serve the public and was more of a PR mechanism for the Fife Health Board. Also that it was actually controlled via the paid workers provided by the FHB, to suit the FHB, and and that ‘unwelcome’ ideas from FHC members or the public were simply bypassed or ignored, even when agreed by the FHC. So, instead, she decided to devote time and effort to StACC and to joining and working for the CAB again, but this time in Dundee.
During June Chris went though about three weeks of feeling very frightened, having panic attacks, and depressed. Largely unable to go out or see anyone. This in turn meant I spent most of my time at home again so I could be with her and try and help. A lot of the time during the day she was too anxious to leave by herself. Fortunately the StACC meetings were in the evening in our local Town Hall. As her condition tended to be at its best in the evenings we managed to go together and she was able to attend her second StACC meeting on the 6th of July. As I wrote in an email to Bob Pollard of Icon Technology the next day:
|
..Things *are* improving, but quite slowly. Like Chris, I've been fighting against the negative feedback effect where; "Feeling worried makes it hard to do anything, and not doing anything makes you worry..."
I was able to ease Chris into going to the Community Council meeting last night. (She was elected last month.) She got involved as I suspected and even asked questions and volunteered for a subcommittee! It gave her a boost to realise that she *can* do these things. (She knows she can, really, as she has been doing similar things for years, but is currently suffering from a total loss of confidence.) Going to the meeting helped her a lot. But it still took us about 20 mins this morning before she was able to walk out with me and go down to the corner shop to buy a box of milk. Progress is 'two steps forward and one step back'... in a zig-zag at times, as well. :-) We'll get back up speed eventually, tho'. I am now able to write some of the research things that're needed and it looks as if no deadlines are gonna be missed. This is helping me to relax and become more able to get on with things... |
Once she had begun to go out again, Chris’s condition improved and she was happy and busy again by mid-July. The problem when she was ‘down’ was getting the process of recovery started, and in particular, getting her to feel able to go out and meet people, etc.
Having initially reviews Icon Technology’s technical document processor, !TechWriter, in the early 1990s I was by 1998 one of its most enthusiastic users and had established a good relationship with Bob Pollard. He was a brilliant and highly talented computer programmer who steadily developed and improved !TechWriter. I’d essentially become an ‘alpha tester’ suggesting ideas for improvements and helping to find buglets. As a result we frequently exchanged emails and I was sent test versions with new features to try out. During the late 1990s many of these developments were to improve the HTML export from !TechWriter. But by this time I was also working with him to add the capability to embed Java applets.
|
Once she had made arrangements to begin the Dundee CAB training course Chris wrote a letter to the FHC formally letting them know she was now planning to resign from its committee. After she had ceased being a member their Deputy Administrator, Lynsey Davidson, came to see her and presented her with a farewell gift in the form of a very pretty glass vase, thanking her for the work she had done for the FHC and NHS. The above photos show Chris receiving the gift from Lynsey.
Because Chris had been going though some very difficult periods I decided to arrange a special surprise for her birthday. She’d been out in the morning in Town and we agreed I’d come meet her for lunch together. I then arranged that Williamsons, the taxi firm we always used, would provide a Daimler. The driver picked me up in this and we then met Chris and took her in it to a lovely hotel/restaurant, Rufflets, just outside St Andrews. The driver had put on a chauffer's uniform to look posh, opened the door for her, and added in a tour around town in the Daimler so she could enjoy being treated like a grand lady out for a drive.

The above shows some views of Rufflets garden.
|
It was a lovely day and we enjoyed an excellent lunch at Rufflets, a walk around their gardens, and then another ride home.
A few days later I got an unpleasant surprise when Dave Walker sent me an email which made plain that he was now very unhappy and that things at Acorn had taken a dramatic turn. In confidence he told me that it looked likely that their ‘workstation’ plans were going to be binned. People would probably be ‘let go’ and that he was already starting to look for a job elsewhere! For those of us who used Acorn computers this was alarming news. But I couldn’t at the time mention it to anyone else because I’d been told in confidence. In the days that followed rumours were starting to go around, but all I could do was express my concerns. Later on Dave phoned me to say he was certain that Phoebe wouldn’t ever appear, but again I couldn’t tell anyone until after the deed was done and announced. There followed a long period when various interested parties tried to arrange a way forwards and ensure future RISC OS hardware was developed and brought to market, albeit no longer by the old Acorn company. Fortunately, this did succeed, but that was no consolation to the people who’d worked at Acorn only for their own project to be binned, and jobs lost.
In September Duncan Robertson began to lose his patience with the way the University and research councils treated him. The reality was that the project to develop mm-wave systems for volcanology was almost entirely his work, with me just helping as and when I could. Yet he wasn’t allowed to either submit a grant proposal or be regarded as a Principal Investigator, and thus obtain funding for a multi-year project whose management and output could be clearly seen as his work. Instead I was required to act like a sort of ‘front man’ as the academic in charge. He was working very hard long hours on this project and various other projects for DERA, etc, yet not getting the credit or treatment he deserved. As a result it was becoming increasingly likely that he would decide to leave and work elsewhere. Which would probably mean the end of the volcano instrumentation project and a number of bits of work for DERA.
Another potential problem that was beginning to loom over our work – almost literally – was a grand scheme by the University to build what came to be called the ‘Gateway’ facility on the North Haugh near the physics dept. This was an example of the kind of project much favoured by politicians and bigwigs. A big, expensive, fancy building they could stand in front of and proudly declare ‘open’ as a sort of monument to their brilliance. The snag for us was that it was going to be built in the line of sight we used for our work on mm-wave remote sensing applications. As a result it threatened to handicap projects like Battlefield systems, volcanological scanners, and another application area Duncan and I were becoming interested in – atmospheric measurements. The new building wouldn’t totally ruin our plans, but would make testing and development more difficult.
On November 8th 1998 Duncan and I went to an ‘Acorn Show’ held at the Marriot Hotel in Glasgow. Initially we’d just planned to go and see the items on show and chat to people in general. However following the dramatic changes at Acorn I’d arranged to meet Dave Walker there and record a conversation with him about Acorn as a document about its history. Before going I’d assumed this might only last half an hour or an hour. But once we got started the discussion continued, and a number of other people joined in. So the end result was a three-hour audio recording covering a wide range of topics from the details of never-to-be-released hardware to Sophie Wilson enjoying ‘pantomime’ at Acorn. Quite nice to hear given my own ‘panto’ involvements back in the days when at QMC...
A problem was that at the time Dave didn’t want all the details we covered to be made public because events were too recent and raw for many of those involved. So the recording sat in my home until recently. A copy has now been sent to the Center for Computing History in Cambridge where I hope it will be preserved for future access by those interested in UK computing history. It is perhaps a testament to the work done by Acorn that, even now, I am writing this webpage and processing images for it, etc, on one of the many examples of an ARM powered RISC OS computer which has been developed and sold since the demise of Acorn. And there are probably more ARM processors in the world today than any other kind. Acorn may not have benefitted in the end, but the rest of us have, even billions of people who’ve never heard of Acorn.

|
In late December we held the now-traditional group Christmas party at the ‘Vine Leaf’ restaurant in St Andrews. The above shows some mug-shots taken at the party. Top left are Fritz and his wife Cath. Fritz was the Physics Dept glassblower, and his work was vital for Natalie’s projects which needed glass containers tailored for the antennas and plasma her systems required to operate correctly. Top right are Duncan Pryde and Duncan Robertson. Duncan Pryde had joined us as a new PhD student in the summer. Bottom left is Graham Smith, the mid-bottom photo is of Natalie Ridge, and the bottom right shows her partner Tony, Chris, and myself. I still claim that neither Graham nor I were actually as drunk as we look!
Tragically, 1999 started with shocking surprise when I was told that Peter May, one of my research students, had died whilst away at home over the holiday period. This was totally unexpected and very sad. He was an outstanding research student and clearly very bright, with a great sense of humour. He had worked alongside Duncan Robertson on the NATO CID project and had done excellent work so I’d anticipated he would have a very successful future. He was certainly a great loss to the group, and sadly missed.
By 1999 the long periods of anxiety about it being safe to leave Chris by herself, and keep up with all the work had started to affect me quite badly. These days I guess the condition might be described as a form of ’traumatic stress disorder’ because I spent almost all the time in a state of anxiety, worrying about what might happen at any moment. The main result was that I developed an increasing level of worry about travelling or being away from home. Provided Chris wasn’t in a ‘down’ or having a burst of severe fits I was able to go to the Physics Dept to give a lecture, attend a meeting, or discuss work with the members of the mm-wave group. But I was starting to avoid having to travel much further, or be away from home for any longer than was absolutely necessary. Going out with Chris was easier, so we often went out for a meal or to see a show at The Byre theatre. And – as with Chris during her bouts of anxiety – once I did get out the door and down the path I tended to feel much better. But that first step was becoming the big one.
At the start of April 1999 Chris had to spent a few days in Stratheden mental hospital, just outside Cupar. She’d become very anxious, confused and seriously depressed and it had been decided that she should be admitted for a while for observation and a chance to rest. Afterwards she had little memory of the episode. However by the middle of the month she was quite active again, going to meetings, and out with friends, etc. She had also started a course of HRT which seemed to help stabilise her feelings, reduce the anxiety, and also reduced the number of fits she was having.
However during April Duncan decided that he would leave St Andrews to take a job at RACAL. This was a bitter blow to me, and I know he did it with great reluctance. But I could fully understand his decision because I knew how unfairly the University and Research Council behaviour treated him, and that my increasingly limited ability to support his work was leaving him with an excessive workload. We’d tried a number of ways to get his status improved so he could take more control and be given the credit, etc, for his work, but the system boxed him in. In some ways the University decision to build the ‘Gateway’ right in the line of sight we felt we needed for much of our work was the last straw. But overall he justly felt over-worked, under-appreciated, and that career development was impossible at St Andrews. He therefore left at the end of April 1999, although we remained in contact as I did hope that things might change for the better in the future. At the end of May we submitted the second proposal to build an imaging system for volcanology, based on Duncan’s work and the advice of a panel of volcanologists who were keen to see the instrument built and be able to use it.
Duncan and I had also started conversations with DERA, the Rutherford Lab, and the Radiocommunications Agency about using mm-wave systems to investigate atmospheric ‘scintillations’ which tended to limit the performance of communications links. With the rise of the internet and the use of mobile phones a rapid expansion of the communications network was under way. One aspect of this was that many more microwave links with greater data transfer capacity were needed. It was known that weather could degrade and limit the data rates provided by such links. But there was a lack of data on the problem or how to optimise performance as people started to use links operating at higher mm-wave frequencies. The plan was that Duncan Pryde’s PhD project work would in due course enable him to work on atmospheric scintillation systems.
Chris continued to experience periods of days-to-weeks of feeling suicidally depressed, anxious, confused, along with fits that included becoming terrified, shaking, etc. Her GP and neurologist kept changing her medication in the hope that it might help, but so far as we could see this was pretty much guesswork on their part. And often seemed to be little more than shuffling the deckchairs in the vain hope of finding a pretty pattern emerged. Chris would see one medic or another most weeks, often seeing two different ones in a week, or the same day! For her ‘routine’ visits to her usual GP I often did not go if she wasn’t feeling too bad, and although we had become disillusioned about expecting them to actually help, we continued to assume their advice was well founded even if they didn’t know what would help.
During July another change to her medication was tried, and we now think this began a chain of events which lead to severe consequences. The CPN (Community Psychiatric Nurse) and GP suggested she start taking a beta-blocker, presumably thinking this might help her to feel calmer and thus reduce her severe anxiety attacks, etc. This was accompanied with some other minor changes to Chris’s medications which included HRT and her various anti-convulsants. For some weeks we experienced a period where we both felt fairly well, and we took a trip ‘down south’ to visit friends and family

|
We spent a few days staying with my Mother and Arthur. The upper pair of photos above show them at their home in Rayleigh. When we visited we noticed that my mother was wearing a wig and that most of her hair had fallen out. She admitted that she’d not been well, but didn’t say too much about the nature of the illness. We also visited Chris’s Aunt and Uncle – Iris and Ted. If you have read some of the earlier sections of this ‘biography’ you will probably already have seen some photos of Iris and Ted’s amazing garden. The lower pair of photos show another part which weren’t previously pictured. In addition to being a very long, multisectioned garden it had a side strip which they had left as mowed grass. The tended part with many trees, bushes and flowers took up just over half of the total area of the garden, and beside it was this grass strip. Between the two was a drainage ditch with a small wooden bridge. These photos give a better idea of just how remarkably long their garden was. Beyond the wire fence was one of the fields of the adjacent farm.
Unfortunately, despite the changed medication, during the weeks after we came back home Chris had more fits, not fewer than before. And she had more periods of being unwell with no sign of any reduction in the intensity of her anxiety, confusion, or depression. On the 24th of August Chris had a major fit at about 8pm. This included all the classic signs of a ‘grand mal’ fit – foaming at the mouth, convulsions, etc, followed by repeated attempts to get up and walk about, only to fall over unless caught. Such fits were generally rare for Chris, typically only about once a year and are the kind of fit most people think of when epilepsy is mentioned. Nearly all of Chris’s fits mainly consisted of being confused, frightened, and behaving like a sleepwalker. These occurred many times a year and we referred to them as ‘minor’ to distinguish them from the more serious ‘major’ grand mal fits.
She visited the GP the next day (25th) and it was decided that she should stop taking the beta blocker that had been started a few weeks earlier as it seemed to not be helping. She was also told to stop taking one of the other medications she’d been trying, having had its dosage halved a couple of weeks earlier. On the 26th Chris had seven minor fits, spread out from 9am to 8:40pm, and was confused and anxious for most of the afternoon and evening. On the 27th she had ten minor fits. The first being at 2:50am and the last at 10:30pm. There may have also been other fits during the night which we both slept though. She was confused and docile all day as if half-asleep. On the 28th she had at least 8 more minor fits. There may well have been others during the night, and whilst I had to go shopping between 10am and noon, unavoidably leaving her alone at home. She also went upstairs to rest in the afternoon and may have had more minor fits then which we didn’t notice.
Consultation with the GP some weeks before had caused us to reduce the daily dose of her main anti-convulsant – Lamotrigine. Given all the fits we decided to increase the dose again back to more like its earlier levels. Chris’s behaviour all day on the 28th was very confused. It was possible to have a conversation on the “Would you like a cup of tea?” level and get a yes or no reply. But not much beyond that. To keep occupied we sat and watched TV together and she kept repeating a series of the same odd phrases like, “What we can say is limited by the sound”, and “Everything is atomic”. When asked what she meant she would refer to “breaking a mirror”. I had the impression she was mentally wandering in a dream state. Confusion like this was common for, say, half an hour or so after a minor fit. So I assumed this state was simply the after effect of having so many fits in quick succession. On the 29th there were no fits, but Chris’s behaviour continued to be confused and strange, and she seemed to have no memory of what she had done more than a few seconds after any event. As a result I was having to check and remind her to take her medication at the correct times because she would otherwise forget. Indeed, she would not have eaten if I hadn’t cooked the meal and then kept reminding her to eat it. She did get up and try to make breakfast, but just stopped and gazed at nothing, laughing occasionally. When I asked her how she was she said “Bliss” or “In heaven”.
Up until the 29th I hadn’t phoned either the GPs nor called an ambulance because I’d assumed the problems were down to a burst of fits. If we had called an ambulance or the surgery for every fit over the years we’d have been able to claim a “frequent flyer” discount because they were routine! So instead we’d learned to deal with them as part of normal life. However by now it was clear this was unusual and serious, so I phoned the surgery at about half past ten in the morning of the 29th. I spoke to a GP who wasn’t Chris’s usual doctor. He agreed that the increase in Lamotrigine dose to its previous level should continue. He also suggested a small dose of aspirin because I’d had flu a few weeks before and Chris had a slightly increased temperature.
On the morning of the 30th Chris seemed to have come out of the “bliss” state and was happy to sit and read a book. She went upstairs for her usual afternoon nap at about 2:30pm and came down again at 6pm to have dinner. But she was now back into the weird ‘dream’ state. Once again repeating the same phrases. She agreed to go upstairs and change from her nightdress into day clothing to eat dinner. But shortly afterwards I heard her come down again, and found her in the kitchen rocking forwards and backwards. When I asked her what she was doing she replied “you know!” and when I asked again she said she wanted to go dancing. She kept rocking and didn’t respond when I spoke. I then dialled 999 and called an ambulance because I had no idea what to do.
The ambulance crew arrived quickly and stayed with her as she continued to rock and ignore questions or suggestions from them or me. A GP arrived (again, not Chris’s usual one) and the ambulance crew left. By this time Chris had gone and sat at her computer. The GP checked her temperature, blood pressure, etc, and they were normal. She didn’t seem to be in any immediate danger, so eventually the GP left. Shortly after that I was able to get Chris’s attention and we watched TV for about 20 mins and then I cooked dinner and we ate together. Later on she went and sat at the computer, but wasn’t actually using it. Nor showing much sign of paying attention when I spoke to her. However I managed to get her to take her medication and get to bed later on.
On the 31st we had a previously arranged appointment with Duncan Davidson, her epilepsy specialist at Ninewells. So we went there by taxi because Chris was still absent and docile. Chris didn’t really understand what was happening at the consultation, so Davidson sent us for her to have an EEG to check. This showed no sign of continual fitting or other problems, so we came home again. By the evening Chris was able to read sections of the newspaper or a book when I suggested she try reading, but was still confused and didn’t really understand what she’d read. She was able to watch some things on TV, but with obvious difficulty. She found cartoons easier to watch than other types of programme. For something like a film or news or other TV programme she would turn her head so she couldn’t see the screen and that apparently made it easier for her to listen to what was said. When I asked about this she’d say something like the picture being too “hot” or “fast” and clearly found complex moving images confusing.
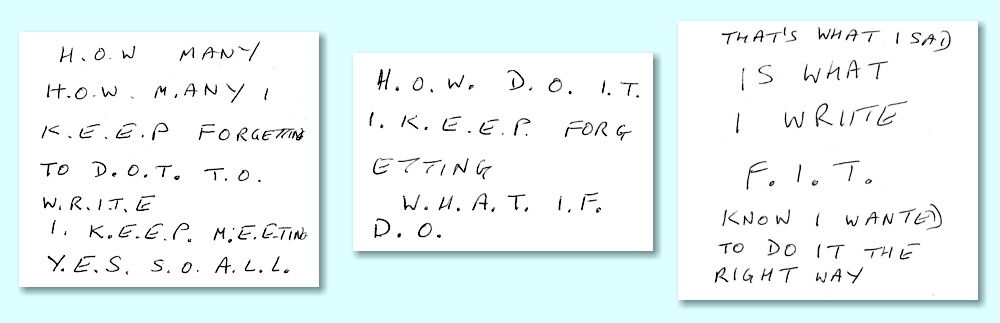
During the night Chris seemed not to get much sleep. From the early morning of the 1st of September she would laugh gently every few minutes. She understood when I said she should try to stop this and get some sleep, but said it was “hard to stop”. Behaviour during the day was similar to before. However around 3pm it became clear she was now able to understood what I said to her, provided I spoke very slowly. However she could not speak sensible in reply and kept getting words wrong or repeating them. She began spelling out words on bits of paper, very slowly writing one letter after another, pausing between letters. She wasn’t able to read letters from a newspaper but when questioned. said it wasn’t because she needed glasses. The positive outcome was that we began to re-establish communication, but she still tended to forget things after a few minutes unless reminded. This was when it first occurred to me that she might have had a stroke. None of the GPs, etc, had suggested this idea, and I knew almost nothing about stroke, but from what little I did, it seemed to fit the symptoms.
Later in the afternoon she started saying “A... B... C...” a few times. Then she said “alphabet” and I wondered if she might like to try playing her favourite game, Scrabble, on her computer. So I asked and she nodded. She was able to switch the machine on and get the game started. (This was actually quite difficult because it required the player to look up a random word in the handbook to enable play to start. Something she did without any problem despite the general struggle she was having with printed words.) Things continued to improve and she responded increasingly well to questions or suggestions, but couldn’t speak to reply. At this point I said, “OK, I know you’re in there and can understand me, but you just can’t say the right words to answer.” Hearing this she produced a huge grin and she flung her arms around me to give me a big cuddle.
|
A little while later she started waving her right hand and I realised she was mimicking writing, so I gave her a pen and some scraps of paper. She took these and started writing things and trying to respond to what I said. This seemed much better than speaking although still quite confused. It made it easier for her to make more appropriate responses. She had to write very slowly. taking about 5 seconds per letter, and often carefully putting a dot after each one. But what she wrote let her reply to questions and explain what she was thinking or feeling.
It seemed that we had made progress. But unfortunately things got worse after we lay down to go to sleep at about 10:30pm that night. She had gone into a mode of saying something every 20 - 30 seconds and found it impossible to stop. I’d say to her something like, “Stop talking. relax, and go to sleep.” She might reply “OK” or “Should I stop talking?... yes I should.” But she’d then speak again 20 - 30 seconds later. What she said became increasingly rambling and repetitive. By about midnight she got up again and went down to her computer and tried to play Scrabble again. This time unsuccessfully as she couldn’t manage to get it working. I kept trying to persuade her to come back to bed, or at least relax on the sofa, but she insisted on staying at her computer, trying to make Scrabble work.
At about 00:30am on the 2nd I phoned the surgery and a GP came to see her. Whilst the GP was with us Chris seemed more subdued and relaxed and it seemed to wake her up. But shortly after the doctor left Chris went into a pattern of walking around the house. She would walk, then stop and say a few words, then walk a few steps, then stop and say a few words. Again stopping to say something odd and occasionally repetitive every 20 - 30 seconds. On occasion she would actually walk backwards for a short time between saying anything. I phoned the surgery again at about 4:30am and discussed the situation with a GP there. We considered the possibility of hospital admission as I was becoming exhausted by this point and it wasn’t clear what I should do. However we decided to delay a decision until the morning.
Chris continued as before until about 6am when I finally persuaded her to come to bed and try and sleep. However we woke up again at 7:30 am and she went down to use her computer to ‘play Scrabble’. Once downstairs it was a mix of her sitting at the computer and doing the walking-talking repetitions. I did at one point switch off her computer entirely as she hadn’t managed to actually start up the Scrabble game, but she didn’t seem to notice this. At about 8:30am I decided that going to hospital would be best and I phoned the surgery again. Her GP came and saw her just after 9am. She then phoned for an ambulance to take Chris to Stratheden mental hospital for admission.
Our neighbours on one side at the time were Joe and Wilma. Joe ran a well-known St Andrews plumbing company. They were very good neighbours and had known us for many years. Wilma came in and sat with me and Chris whilst we waited. Although Chris was apparently unaware of what was going on she did have some kind of weak contact with reality. At one point I asked her, “Chris, can you type something for me?” She responded by pausing and then carefully typing the keys, ‘4’ ‘U’. i.e. “For You”. I then asked her “Can you type ‘hot’” and she typed the keys ‘H’ ‘O’ ‘T’. I did the same, asking for ‘cold’ and she responded correctly. So it was clear that the problems were with communication and memory. She was still ‘in there’. I’d switched off the actual computer, but she was still using the keyboard as a way to communicate!
The ambulance arrived about an hour after it was called. Chris initially resisted being moved until I realised that she was clutching the keyboard. So I unplugged it so she could take it with her. That done, she allowed herself to be put in the wheelchair and carried to the ambulance. Once we got to Stratheden she was admitted and given something to ensure she relaxed and slept for a while. It seemed likely that she hadn’t actually slept properly for many days. Come to that, neither had I! I stayed with her until the mid-afternoon, although a lot of that time she was sleeping. At about 6pm I went home to get some clothing for her and got back to Stratheden just after 7pm. By then she was drowsy, snuggled down to sleep, so I held her hand for about 20 minutes then came home again to eat and sleep.
I went back to Stratheden at 10am on the 3rd of September. (It’s about a half-hour taxi ride from home.) Chris was still quite confused, rambling, and with a short attention/memory span. But she was rapidly improving and the more disordered behaviour of the previous day didn’t reappear. I discussed her improving condition with the staff and the possibility of her going home. As it was a Friday they agreed she could come home on a ‘weekend pass’ to see how we got on. So I went home for lunch, dashed around town to stock up on shopping, and then back to the hospital just after 3pm. During her stay the only difficulty with the hospital was that I had to keep chasing them to give Chris her anti-convulsants, etc, at the correct times because the regime we’d found best didn’t fit in with the standard hospital timetable. But apart from that she was well treated by everyone there.
Chris’s condition continued to improve over the weekend at home. On Saturday morning she was happy to come for a walk down to the seafront – one of our favourite walks. This helped her become more aware and cheered her up. Although she still preferred to watch cartoons to any other TV she started doing small tasks around the house in the afternoon and became much more relaxed. She was also able to read in bed for a short time before we went to sleep. She also happily got up and made breakfast the following morning. In the afternoon she tried phoning her Dad but stopped after about 5 mins saying it was “Too hot”. When I asked what she meant it was that she found having a conversation over the phone was too confusing. However she recovered within a few minutes. And later on played Scrabble, beating the computer three times.
On Monday morning Chris was clearly anxious about going back to Stratheden because her “pass” was only for the weekend. Having spoken with the hospital staff on Friday I assured her that her progress meant they’d almost certainly be happy to let her come home again with me. We decided to go for a walk as doing this had made her feel better the previous day. So we set off again, and once we got to the seafront she suggested we go to the bus station and take a taxi from there to the hospital. So that’s what we did.
When we got to Stratheden, Chris said she’d stay in the taxi and wait while I went in. So I had to explain they’d need to see her, even though it made her nervous. I arranged for the taxi to wait and expect to take us both home again. This was to comfort Chris, but also because I thought it pretty likely they’d be happy for her to come home again given her improved condition. She was a bit confused during the interview with the consultant, but was calm. So after a few minutes he agreed she could be discharged home, and he’d make an out-patient appointment to see her in St Andrews at a later date. Fortunately, Chris’s condition then improved gradually over the following weeks.
For me, the most frightening period was when her behaviour was so weird for many days without an respite. At that time I became really worried that she might never recover and remain trapped by the confusion and memory-less repetitive odd behaviours permanently! So it was an enormous relief when I realised she was ‘still in there’ and trying to communicate, and when her condition steadily improved from the weekend onwards. Her fits and periods of serious depression and anxiety were a worry and a cause of stress, but experience showed they did pass in time, so could be regarded as patches of ‘bad weather’ to be coped with and dealt with until things could be improved again.
Although we didn’t think of it until after events, we now believe the central problem was that Chris actually had a stroke at or around the time when she had the major fit on the 24th of August. But neither we nor any of the medics had realised this. So the closest we got to the recommended early treatment for a stroke was the small amount of aspirin suggested for other reasons! That may have helped a little. However we also now suspect that the stroke itself may have been triggered by the way Chris’s GP kept fiddling with her medication on an almost, “Here, try this!” basis - changes often being made within a week or two of each other. In particular, the stopping of the beta blocker almost immediately before the events of the 24th. Perhaps causing something like a dramatic change in her blood pressure that day. In addition, the dose of one of her other medications, Clobazam, had been reduced and this may have caused her to be losing sleep without us realising how much this was happening. Alas, now we will never know for sure. We only know that it was a really awful chain of events that we can only be glad to have managed to largely recover from. It was a week in hell, but it could have been worse!
The main consequence of the episode was that my attitude to GPs altered. Firstly, I became much more sceptical of the “try this” nature of the way they’d suggest altering medications. Secondly, I became less willing to have Chris see them without my being with her to ask for details of why they proposed a change – so that I could then DIY my own research on what might happen, or why it might be a good/bad idea. I also became particularly aware of the episode showing that they had for days assumed that events were simply a manifestation of epilepsy. No one had suggested a possible stroke during the early consultations or visits, and thus no checks or treatment for one had been even suggested. Later years firmed up my impression that many medical practitioners tend to ‘pigeonhole’ a patent and stick a label on them. Then treat the label not the patient, ignoring signs that the diagnosis isn’t correct. One of the reasons I’ve detailed the events above is in case it helps anyone else in a similar position to recognise what is happening to them or someone they love.
As a result of the above events I took a few weeks off work to help both Chris and myself recover. During this time Paul Cruickshank and David (‘Dav’) MacFarlane joined the mm-wave group. Both Paul and Dav had done undergrad projects with the group in the two previous years. They both had now graduated with the top two 1st’s in Physics at the end of their final year. I had also managed to get an extension for Duncan Pryde’s PhD studentship support and he had taken on some of the work which otherwise would have been done by Duncan Robertson. As usual, Paul and Dav’s initial work was aimed at allowing them to get a more general idea of what the group did, and what might suit them best. However since they were already familiar with the group this developed into an arrangement where Paul worked for Graham, and Dav worked on the topics I was trying to push forwards.
By the last few months of 1999 discussions were under way to arrange a project to monitor atmospheric effects using instruments we proposed installing on the roof of the Physics building. Both the Radiocommunications Agency and the Rutherford Laboratory were keen to make progress with this. Alas, out second attempt to obtain an NERC grant for volcanological instrumentation was also rejected. This was for various reasons, but the central problem was that the relevant committee and referees didn’t really understand what the mm-wave measurements would actually be able to do. So the challenge was to explain, and convince them that we knew what we were doing. However Duncan Robertson had left St Andrews, Chris was often unwell, and I was frequently unable to travel to meetings to help answer questions or explain details. The people we were co-operating with at Lancaster University were very keen and helpful, but they weren’t experts on mm-wave systems. We had managed to arrange that a well regarded volcanologist, Peter Francis, had investigated what we proposed and he was happy to support the proposal. But tragically, he died shortly before the relevant decisive meetings took place. So the second attempt to get funded ran into a series of major barriers. Fortunately, we tried again in later years and the photo at the top of this webpage gives away the fact that – eventually – we succeeded. That’s a story for a later time, however...
The one really excellent item of news was that during the first week of November 1999 Graham Smith was almost simultaneously awarded a lectureship at St Andrews and a Senior Fellowship! Following on from this, Paul became his research student and they worked together on the development of mm-wave ESR-based measurement methods.
One consequence of Chris’s ‘down’ periods was that I tended to work at home as much as possible so I could be there when suddenly needed without warning. I tended to write reports, teaching material, web pages, and magazine articles as a way to keep myself occupied and take my mind away from being worried about Chris being unwell.
By the middle of 1999 I’d written a number of articles about Acorn computers and software. These appeared in various magazines, most notably ‘Archive’ which was (and still is!) in effect a ‘fanzine’ for Acorn/RISC OS users where they could exchange ideas, programs, etc. One result of this was that I’d been contacted by the editor of a professional magazine called ‘Acorn User’. Since I was known in the Acorn community as being keen on the technical document processor, !TechWriter, he asked me to write an article about that and promised to pay me the grand sum of three hundred quid for the article. This seemed good timing because the programmer developing !TechWriter – Bob Pollard – and I had become interested in having it support active Java programs to provide interactive graphics in a !TechWriter document and when exported as webpages. So it seemed an excellent chance to reveal this to readers. I therefore wrote the article, sent it in, and it was accepted.
|
The article appeared some months later in the issue of Acorn User (AU) cover-dated September 1999. The above shows some snippets from what was printed, and the magazine cover. For an author who has to include a lot of mathematics !TechWriter is superb because it makes typing (and editing or altering) the equations easy, and it lays them out beautifully and in accord with the standard rules for mathematical typography. The addition of Java support was, at the time, also impressive as it allowed authors to illustrate their work in an way which readers could use to explore the results of a given analysis. Sadly, by the time the article appeared two problems had become evident. Firstly, the development of Java for the Acorn/RISC OS platform had essentially stalled. It had become a casualty of the changes at Acorn. The second was that, despite repeated inquiries and requests, I’d not been paid for the article as promised!
Now I was quite happy to write articles for no fee when I felt that was justified and worthwhile, and had done so for Archive. But the editor of AU had contacted me and commissioned me for an offered sum to write for his magazine. So I felt that such a promise should be honoured. My initial inquiries had generated responses which basically kicked the can down the road. But finally the editor phoned me and said he couldn’t pay. Then and in later discussions he said that he wanted the money to offer to other potential authors, and if I insisted the magazine would simply cease publication. This really bothered me because to me it sounded like the same process was being applied to a succession of authors. And although I’m not a lawyer, seemed to me like a sign of “trading whilst insolvent” which I think is an offence in the UK. In the end I settled for a letter signed by the then-editor stating in writing that Acorn User did NOT own any of the copyright for the article, and thus could not reprint it, nor sell it on. I have wondered, since, how many others may have been treated in the same way.
|
On Wednesday 15th December we held the group’s Christmas dinner at the Vine Leaf as usual. The photos above show the ‘crew’ at the time. From left to right: Dav, Duncan Pryde, Graham, Chris, and Paul. The evening was enjoyable, but it had been a really bad year in many ways. So the main thing we had to celebrate was that we’d survived!


[ N.B. The images marked with ‘CC’ on this webpage were derived from the “Wikimedia Commons” set at https://commons.wikimedia.org/wiki/Category:Soufri%C3%A8re_Hills ]